I had an episode of IT band pain, and I cured it. Here’s how:
I was running with some trail runners last February in Marin County, and I was feeling a little bit ambitious, so I decided to push myself and keep up with some runners who were way out of my league. It was me, my wife, and two other ladies who happen to trail run long distances for the fun of it, and also happen to be accomplished ultra-runners. Way out of my running league. Both would since go on to finish the Lake Sonoma 50 miler, so that’s the caliber of runners I was trying to keep up with.
So in Point Reyes National Seashore, along the Bear Valley trail, we all set off. I was proud that I was keeping up with these long distance runners, as they run slow and steady. I am more of a habitual sprinter, so I did pretty well keeping up in the beginning. But once we got just past the halfway point, and at 11 miles, I felt an unfamiliar pain in the side of my left knee.
This pain felt like it was exactly in the joint line of my knee, which worried me. But, it was also just past the joint, and just above the joint. I felt it bad with every step I took downhill, and as I hobbled back to the cars to finish the race, I started to feel it with every step. It was crippling.
When I got home, I cracked open my orthopedic textbooks to go over some differential diagnostics. Was the pain from a meniscus? Was it from the lateral collateral ligament? I realized that is was biomechanical pain, so I wasn’t worried, but I didn’t know exactly what was causing the pain. It was then that I realized that I was hit with the famous IT Band Friction Syndrome.
 IT Band Friction pain happens when your knee is flexed at about 30 degrees, and you are placing a load on your IT band (IlioTibial band.) If your IT band is repetitively irritated in a certain way at a certain angle, and at certain loads, it will start to hurt. Believe me, when it starts to hurt, it can hurt in a big way.
IT Band Friction pain happens when your knee is flexed at about 30 degrees, and you are placing a load on your IT band (IlioTibial band.) If your IT band is repetitively irritated in a certain way at a certain angle, and at certain loads, it will start to hurt. Believe me, when it starts to hurt, it can hurt in a big way.
Part of the public myth of the IT band is that it gets “tight.” This is not true, and I’m going to explain to you what I’ve learned when I was going through this pain. And, I’m also going to explain to you what I did to rehab it and cure it, because I had a 22 mile trail run in Calistoga I signed up for that I was going to do a few months after my injury.
Your Loose & Squeaky Suspension
It turns out, when you have IT band friction pain, it’s not from a tight IT band as most people would like you to believe (just roll it out!) IT bands have been measured to be too loose on people with pain from IT band friction. Yep. If you have IT band pain, you’re not being supported enough by your lateral hip stabilizers. As a matter of fact, the pain might not even be from repetitive friction, but it could rather be from the band pulling away from the sensitive periosteum lining of the bone.
As I did my research, and I was finding out that the best way to cure an IT band problem was to strengthen your hip muscles, I also found some research that found that if you have IT band pain, you’ll also have less tension placed on your IT band. It’s not too tight, it’s too loose.
The thinking is this: If your car had a worn out, squeaky suspension, you’re going to eventually cause premature wear in other parts of the suspension, because the whole geometry is being thrown off. The IT band is part of your body’s suspension system. With every step you take, the IT band absorbs and stores kinetic energy to be released a second later in another part of your gait cycle. You take a step, energy from the step travels up your leg to your knee and bent leg. The step energy gets absorbed partially in your thigh in the ligament that surrounds and supports your thigh and pelvic muscles. This is the IT band. It provides tensile support when you walk or run, and it is a hybrid battery that stores energy temporarily for you own performance.
With weakness in the hip muscles, women tend to drop a hip when they run. This loss of core stability at the pelvis causes the trunk muscles to let go, and one hip will drop. In men, weakness in the core stability of the pelvis will cause the thigh to rotate to the inside, and the knees will go bow-legged.
If you’re walking around with weak, unconditioned glutes as I was, then something is going to wear prematurely. Your hip will dip, and your knee will buckle under load. For me, I wasn’t conditioned at that time to run those steep hills more than 11 miles, and my legs paid the price for months to come.
A Plan For Recovery
Since I’m a smart enough clinician to solve problems in the body, I know that I had to access the world’s knowledge for best practices for IT band knee pain. If you have knee pain, you could look right at the painful spot-the knee, and concentrate your efforts there, but that is only looking at the warning light, but not the faulty parts.
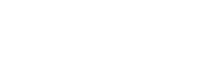
The most important, evidence based approach to IT band disorders is to right away strengthen those muscles at the hip that influence the band. This includes your tensor fascia lata, the gluteus medius, and the gluteus maximus. These three muscles are instrumental in keeping your IT band nice and tight and well conditioned to stay away from trouble. Even thought the gluteus medius doesn’t directly attach to the IT band, it plays the most important role in controlling your pelvis and hip architecture to save your IT band.
My weapon of choice for gluteal rehabilitation was to use an elastic fabric loop called a hip circle. This loop is designed to go around your knees to restrict and train hip and thigh abduction-or kicking your leg out to the side. My favorite way of doing this is to just stand on one foot while kicking the other foot out. This causes your hip muscles to immediately protest in burning pain, but it’s tolerable, and it’s rehabbing yourself, so you do it. I bought some bands for home, and I already had one at work. I wanted to get this done several times per day.
These muscles hold your pelvis steady, and they tighten the reins of your IT band, so everything is well supported. But what about the pain in the here and now? I couldn’t even walk down stairs, and I’m really good at taking stairs. To support this area I did two things at the site of the pain. I used medical tape to strap down the insertion of the band at Gerdy’s tubercle on the Tibia, and I taped the “friction” point of pain on my femur at the lateral epicondyle. I packed that leukotape down tight just so I could get around with less pain, and I even strapped it on for my follow up 22 mile run.
The other thing I did at the site of the insertion was some shockwave therapy. I had just gotten my shockwave machine, and I knew it would be a valuable treatment modality because it would do two things for me. The first thing it would do for me was that it would have an analgesic effect on the site of pain. Even though it would be a temporary effect, I was welcoming any kind of pain relief. The other thing it did for me was that it would stimulate the healing process. Shockwave therapy stimulates the release of growth factors in injured tissue. Shockwave converts mechanical stimulation into the biological release of growth factors for tendon repair. Shockwave therapy can even help with non-union bone fractures, so I know it would be worth a shot.
One of the important things that I did away from the site of pain was probably just as important as exercising my stabilizing muscles: I got adjusted. For 2-3 times per week, I would ask Dr. Luck to adjust my pelvis and my feet and ankles. I wanted my pelvis to be symmetrical so the muscles supporting the swing and propulsion of my gait would fire evenly. You don’t want to run through your world with muscle imbalances between your low back and your legs; you want them equally strong.
Likewise, I wanted my feet to be flexible, I wanted my ankle bone to move about its proper axis, and I wanted my heel bone to remain in a neutral position. Having all 26 bones in each foot move well and with good alignment helps the gait mechanism. Part of the gait mechanism that happens with every step you take is called the “Windlass Mechanism” When you toe-off to move yourself forward, flexing your big toe causes your arch to firm up and go ridged. This also goes up your leg to cause your knee to rotate and screw-home for more concentration of power. This, at the knee, can influence the way your IT band is angled. So, I knew I had to keep my foot and ankle biomechanics on point.
Even though I started in with the best practices of tendon rehab right away, it was a long journey to make the pain go away. The injury happened to me in February, and my records show that my Calistoga run was in April, and I was still hurting, but not as bad. It was a slow steady improvement, and by the time June rolled around, I was probably again at my best, and I could again run downhill without anything bothering me.
As I reflect on this, it makes me grateful that I have these painful experiences because it better helps me understand and have empathy for what my patients go through. I also feel guilty that I might have had hundreds of patients in the past where they might have had the same exact thing going on, but I didn’t fully understand their suffering and what they could have done to get out of it faster. I don’t take IT band pain for granted anymore, but please, I no longer need empathy for this problem again. Once was enough.